Since the #AccessforAll campaign launched in 2019, we have seen considerable success with five provinces and one territory introducing new coverage for Continuous Glucose Monitors (CGM) and Flash Glucose Monitors (Flash GM). As a result, thousands of Canadians living with type 1 diabetes (T1D) have been able to access this diabetes technology, reducing individual out-of-pocket costs considerably.
For 2022, the campaign is focusing on persuading the Atlantic provinces to also begin providing this much-needed coverage. Armed with additional data from a new cost-effectiveness study, as well as successful models from other Canadian jurisdictions, we are confident that we’ll be able to welcome more good news in 2022.
We began the year with a productive meeting with the Minister of Health in Nova Scotia, The Hon. Michelle Thompson. We discussed the benefits of offering coverage for Nova Scotians living with T1D, and potentially expanding the insulin pump program to those older than 25.
Mother and daughter, and JDRF advocates Amanda and Aaliyah Williams spoke to the Minister about how important patient choice is for those living with T1D. Aaliyah, who is 14 years old, shared how she initially started using a different advanced glucose monitoring device, and soon realized that it wasn’t working for her. Luckily, because she is covered by private insurance, she was able to make the switch to the device that helps her live a healthier and safe life. She has never been happier, but not everyone is as fortunate to have private coverage, and this is why we are urging the government to step up and fill those gaps.
Leah Sutherland, a mother of a young adult living with T1D worries for her daughter who will age out of pump coverage next year. Leah’s daughter is at a critical point in her life, starting her career and not in a position to take on the cost of a pump and supplies, as they cost thousands of dollars per year. T1D does not end at 25, so Leah has been advocating tirelessly on behalf of her daughter, collecting signatures for a petition that will be presented in the legislature in the coming months.
We were also encouraged by PEI’s commitment to diabetes funding in their 2021 provincial budget. We, presented to Minister of Finance The Hon. Darlene Compton to make the case for CGM/Flash GM funding, and made a similar appeal to the Minister of Health in Newfoundland, The Hon. John Haggie.
We look forward to working with the Atlantic provinces to ensure that the T1D community is supported in their efforts to increase public coverage for insulin pumps and advanced glucose monitors (CGM and Flash GM). To support the campaign, please take a few minutes to send a message to your representative. You will be voicing important concerns in response to a new era of healthcare.
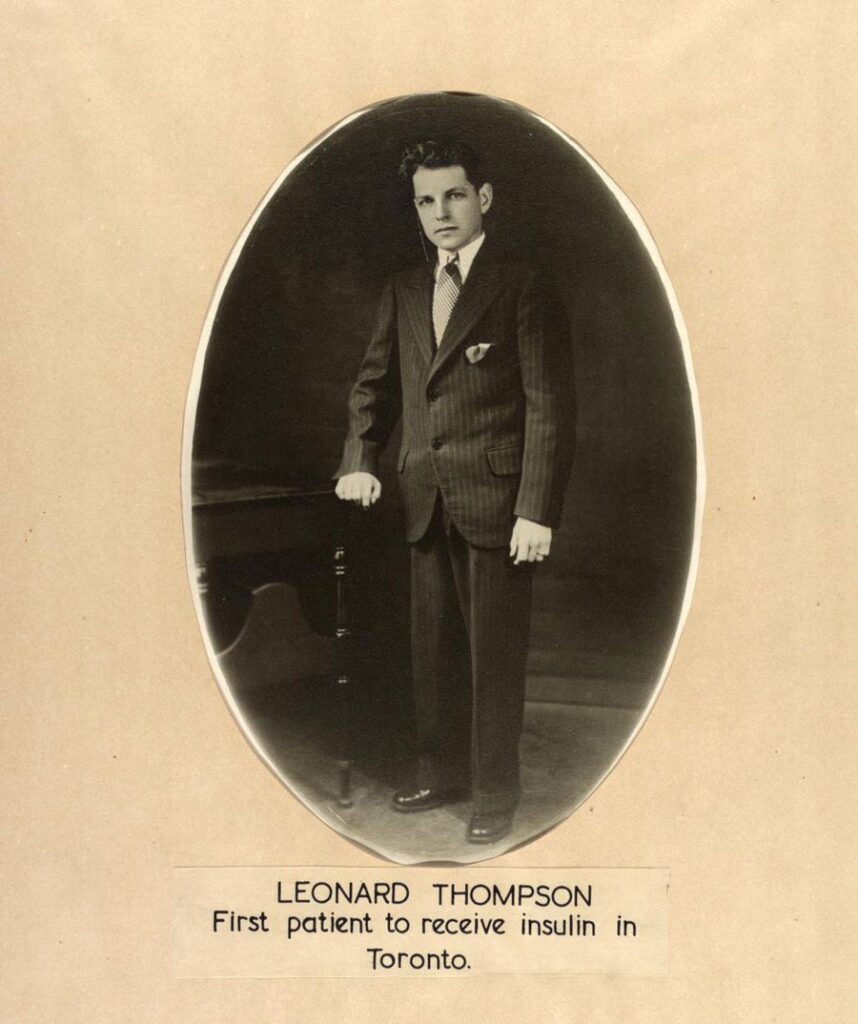
January 23, 2022 is the 100th anniversary of the first successful insulin injection for diabetes in a human. Prior to this, a diagnosis of type 1 diabetes (T1D) meant certain death. On this date, a fourteen-year-old boy named Leonard Thomspon, who was dying from complications of T1D received the first real treatment for the disease. He would live another 13 years. Leonard could be considered the first human in an insulin clinical trial. As a result, millions across the globe can now better manage their diabetes.
This day has special meaning to our family. Our daughter Tilla was just 10 years old when she was diagnosed with T1D in the summer of 2019. Now, like everyone who lives with this disease, her days are a series of decisions, tracking her blood sugar and insulin levels, and measuring her food, particularly carbs. And although we are fortunate to have the best diabetes technology available to us, it can still be immensely stressful at times. It is a 24-7 disease with no days off.
After Tilla’s diagnosis, we started researching available clinical trials that she could be enrolled in, and Tilla bravely rose to the challenge. She enrolled in the PROTECT study, which is testing an investigational medicine called teplizumab – a drug JDRF Canada has supported earlier trials of. It is hoped teplizumab will help people with T1D to continue making more of their own insulin and reduce or even eliminate the need for insulin injections for many months.
PROTECT is a randomized controlled trial involving a placebo group. Despite knowing that Tilla could be placed in the placebo group, we still chose to participate, with the hopes that not only could it change the disease course for Tilla in the short term, but in the future could impact thousands of other people like her who are diagnosed with T1D every year.
Our son Allan is also enrolled in a T1D clinical trial at Sick Kids hospital in Toronto, ON. He has all the antibodies for the disease, which puts him at far greater risk of developing it in the future. Along with his mother, Allan has flown to Toronto twice. He takes one pill per day/ two pills per day on weekends. It is our hope that if he is not receiving the placebo – this treatment might prevent or delay him from developing T1D. And even if it does not, we know that he is still contributing to advancing scientific knowledge of how we might better screen for and prevent diagnoses of T1D.
Being involved in clinical research makes us feel as a family that we are directly and personally contributing to helping find a cure for this devastating disease. And we believe this is an important message. Participation in clinical trials is the only way we can get treatments to market and to everyone who can benefit from them. We consider anyone enrolled in clinical trials heroes.
What many people do not know is that the first insulin injection took place on January 11, 1922, but Leonard Thompson had an allergic reaction to it. And that when that first injection did not work, he took another step forward and tried again. From the bravery of one teenage boy, came millions of people whose lives have been saved by insulin. And every year across the globe, people living with T1D celebrate their ‘insulin anniversary’ while waiting for the next breakthrough in diabetes.
Every person who participates in a T1D clinical trial study helps us get closer to a cure. We recognize their courage and are so grateful for their help in accelerating research that will one day mean a world free from diabetes.
We are grateful to JDRF Canada, whose primary goal is funding the most promising research that will move us beyond insulin and toward a cure for T1D. Their investment in this research means that we can participate in these important clinical trials.
Henrik Karlsson, Anna, Tilla and Allan Karlberg, on behalf of JDRF Canada
Bell annually runs its #BellLetsTalk campaign, raising awareness and helping to combat the stigma surrounding mental illness in Canada.
Living with type 1 diabetes (T1D), whether it’s you, your child, a friend or loved one, has an impact that extends far beyond physical health. The stress of managing a chronic condition, both from the time of diagnosis and even decades later brings with it challenges to overall wellbeing. Mental health challenges are common for people with T1D, at any age.
#BellLetsTalk day is January 26, 2022. We use this day across the country to amplify and recognize the importance of treatment for mental health issues, including for people with or affected by T1D.
Living with T1D
T1D is a chronic autoimmune disease that can be diagnosed at any age, but most commonly in childhood.
People living with T1D must follow a strict lifelong treatment plan that includes constant blood sugar monitoring, counting carbohydrates and taking insulin multiple times a day to stay alive. There is no treatment beyond insulin, and no cure.
T1D can impact mental, emotional, and psychosocial health
Mental health represents one of the most pervasive health issues affecting Canadians today. Combined with a chronic condition like T1D, feelings of anxiety, stress and depression are often intensified.
T1D frequently impacts a person’s emotional, social, and behavioural health, known as psychosocial health. One in five youth with T1D experiences anxiety and, compared to those without the condition, people with diabetes are more likely to experience depression or develop an eating disorder.
Diabetes can feel like a ‘hidden’ disease and isolating and lonely – particularly for kids and teens.
Traditionally, healthcare for T1D focuses primarily on managing glucose levels to help stave off potential diabetes-related complications. The mental health challenges that can accompany the condition are often overlooked, and this can affect overall health.
Many people with T1D suffer what is known as “diabetes distress” – a term describing the powerlessness, stress, guilt, relentless worry, and denial that comes with the constant self-management required to maintain balance with this disease.
We also know that under-served mental health issues can lead to higher HbA1c and an increased risk of complications, yet despite this – mental health care remains a gap in Canadian healthcare for people with T1D.
How JDRF Canada is addressing gaps in mental health care for people with T1D
In January 2021, JDRF Canada launched its $100 Million Campaign to Accelerate, which includes a six-pillar approach to funding research and other programs that accelerate towards cures and improving lives for people living with T1D today. One pillar of the campaign is dedicated to addressing mental health issues and expanding support to the T1D community.
It is an ambitious plan that initially includes five areas of focus: funding research to test psychosocial interventions, providing education about psychosocial issues in diabetes to health care providers, supporting postdoctoral fellowships for clinical psychologists in training, providing support and resources for people living with T1D, and developing and launching a virtual training program about diabetes for registered mental health care providers.
JDRF will also be developing and launching a directory to connect the diabetes community to providers that understand their unique mental health needs.
JDRF will partner with various diabetes and mental health organizations, including those that serve people living with type 2 diabetes
The virtual training program on diabetes and mental health for mental health care providers will begin later this year. If you are a mental health provider interested in learning more, please contact: mentalhealthstrategy@jdrf.ca
Additional JDRF Resources
From diagnosis to daily life years after, having a community and connection to others affected by T1D offers critical support and lets them know they are not alone.
To help foster and grow the T1D community across Canada, JDRF has a strong community engagement team that works to offer the following sources of support:
Our virtual Let’s Talk T1D series, which includes a Connection Series moderated by volunteer with T1D and offers a space safe to share.
Talk T1D – a mentorship program that provides one-on-one support to families who are impacted by T1D from trained volunteers who have been there.
Our Youth Ambassador advocacy program for kids between 4 and 18 who want to share their T1D stories and inspire their communities, increase awareness of T1D, and join hundreds of kids across the country to help JDRF fundraise for a cure.
On #BellLetsTalk day, as we work to reduce the stigma around mental health issues, we recognize that psychosocial and mental health is a key component of overall health and should be integrated into a holistic healthcare plan for all Canadians affected by T1D.
Principal researcher confirms trial participants with a history of hypoglycemia unawareness are now insulin independent.
Funding cell replacement therapies research is one of JDRF’s most critical undertakings globally, in its efforts to support the most promising cure-based research into type 1 diabetes (T1D).
On January 10, 2022, Sernova Corp. provided a progress update on its Phase 1/2 T1D clinical trial, a JDRF-funded clinical trial of its cell replacement therapy. The findings were presented by Dr. Piotr Witkowski, the clinical trial’s Principal Investigator at the University of Chicago.
Sernova is a clinical-stage regenerative medicine company and has continued to demonstrate promising results for its Cell Pouch System™. When transplanted with insulin-producing islets, this system has consistently demonstrated in ongoing trials that it can produce insulin in people T1D, and participants maintain more consistent blood sugar levels. Additionally, it has demonstrated ongoing safety and tolerability of the system. In Sernova’s current clinical trial, patients must take immunosuppressive drugs to prevent rejection of the implanted cells.
Sernova’s approach for T1D involves transplanting purified islet cells (the cells in the pancreas that produce insulin and that are destroyed in people with T1D) from organ donors into the Cell Pouch™, an implantable medical device that allows these cells to survive long term and produce insulin. This is a cell replacement therapy that has the potential to be a T1D cure.
The objective of Sernova’s Phase 1/2 clinical trial is to assess the safety, tolerability and efficacy the Cell Pouch™ transplanted with insulin-producing islets in trial participants with T1D who have a history of hypoglycemia unawareness and severe hypoglycemic events.
To be in the study, participants must meet stringent eligibility criteria including, but not limited to, long-standing T1D, recent episodes of hypoglycemic unawareness and an absence of glucose-stimulated C-peptide detectable in their bloodstream (a biomarker that demonstrates the body is making its own insulin).
Hypoglycemia unawareness is a person’s inability to recognize the symptoms of low blood sugar before they become severe or even fatal. It typically occurs when blood glucose levels are below 3.0 mmol/L and is estimated to affect approximately 15% of people with T1D.
Highlights from the study include:
Maintained and ongoing safety and tolerability of the Cell Pouch™
Islet transplantation to the Cell Pouch™ resulted in the establishment of new, measurable islet function, documented by detectable levels of stimulated C-peptide in the first three participants who completed the course of transplants.
A supplemental, single intraportal islet transplant was enough for the first two participants to achieve and maintain sustained ongoing insulin independence and freedom from severe hypoglycemic events for over 21 and 2 months, respectively.
The third transplanted participant who recently completed their course of Cell Pouch™ transplants and a supplemental intraportal islet infusion, saw improvements in glucose control, near-normal levels of C-peptide, an absence of severe hypoglycemic events and reductions in daily insulin use.
Three additional participants are progressing through the study.
Sernova’s Cell Pouch™ System was created with the goal of one day treating people with T1D and other chronic diseases using stem cell-derived technologies, that will not require immunosuppression. Sernova is partnering with other companies to advance the Cell Pouch™ system to testing using a stem cell-derived source, as well as approaches that will reduce or eliminate the need for immunosuppression.
To date, between our partner organizations JDRF has invested more than $140 million USD in cell-replacement therapy research for T1D. As we celebrate the 100th anniversary in 2022 of the first successful insulin injection, this is another example of Canadian excellence in diabetes research that is accelerating us towards cures.
January 23rd marks the 100th Anniversary of the first successful insulin injection
JDRF’s primary goal is to cure type 1 diabetes (T1D) through research – as quickly as possible. To support people with T1D while cure research is advancing, we also fund ground-breaking research that seeks to make life with T1D easier, safer and healthier. With the discovery of insulin 100 years ago, JDRF is committed to funding the most promising research to move us beyond this treatment and toward cures.
1921
Before insulin treatment, a diagnosis of type 1 diabetes meant inevitable death. T1D destroys the beta cells in the pancreas that make insulin, without which, the body cannot maintain healthy blood sugar levels.
In 1921, Frederick Banting and Charles Best discovered that the pancreas produced the insulin hormone under the directorship of John Macleod at the University of Toronto. With the help of James Collip, they purified a synthetic version of insulin and produced the first real treatment for diabetes. To this day, it remains one of the most important scientific breakthroughs in the medical field, often called ‘Canada’s gift to the world’.
January 11, 1922
On this date, fourteen-year-old Leonard Thompson, a teenage boy who was dying from T1D complications, became the first person to receive an insulin injection. But instead of lowering his blood sugar, it caused an allergic reaction. Leonard’s doctors went back to the lab, where they worked nearly around the clock to improve the formulation.
January 23, 1922
Almost two weeks later, they returned to Leonard’s bed with a new syringe of insulin. With this version, Leonard’s symptoms began to disappear, and he regained his health. He would live another 13 years. The discovery of insulin, along with Leonard’s willingness to try this new treatment meant the death sentence that was T1D could be lifted, and people around the world could use insulin to manage their diabetes.
The importance of clinical trials
Research is how insulin was discovered and it is how we will find the next generation of therapies for T1D, and eventually a cure.
And clinical trials are an essential component of medical research and development. While Leonard’s receiving the first insulin to human injection was not known as a “clinical trial,” at the time, his participation allowed his doctors to rework and refine the formula that would make it a successful treatment for diabetes for over 100 years. In modern terms, Leonard was the first human participant in a clinical trial to test the impact of insulin on T1D.
This demonstrates the far-reaching impact of clinical trials. These studies can help bring new, better treatments to market that will impact the lives of millions. Thanks to Leonard Thompson, the updated version of insulin became a true breakthrough in diabetes care.
Funding cell replacement therapies research is one of JDRF’s most critical undertakings globally, and between our partner organizations we have invested more $140 million USD to date.
JDRF funds stem cell derived beta cell replacement trials that are ongoing right now, like those at ViaCyte, Vertex and Sernova and from here we may witness the research that leads to a T1D cure.
Participating in clinical trials
JDRF is funding many clinical trials, and one of the biggest challenges is finding volunteers to take part in studies – and it’s often because they simply didn’t know they could. It is also important to have a diverse group of participants who represent the Canadian T1D community, so that potential therapies and treatments can be tested for efficacy against the larger group who will be using them. When someone participates in a clinical trial, they help all people living with T1D, by enabling research towards better health outcomes and cures.
Choosing to participate in a clinical trial is a very personal decision. Early access to promising new treatment can be an enormous benefit. Others have found that by participating in a clinical trial, they learned more about their health or T1D management. And it can be motivating to know you are contributing to helping accelerate research that can improve the lives of people living not only with T1D, but other chronic conditions as well.
One person can make a difference – watch Tilla’s story of participating in clinical trials after her T1D diagnosis
On January 11, 1922, Leonard Thompson took a leap of faith. And when that first injection did not work, he took another step forward and tried again. From the bravery of one teenage boy, came millions of people whose lives have been saved by insulin. And every year across the globe, people living with T1D celebrate their ‘insulin anniversary’ while waiting for the breakthrough that will move us beyond insulin and towards a cure.
Every person who participates in a T1D clinical trial study helps us get closer to moving therapies from the lab to the market. We recognize too their courage and are so grateful for their help in accelerating the research that will one day mean a world free from diabetes.
JDRF is committed to providing timely information about the latest research updates relevant to the diabetes community. Early January 2022 researchers from the Centers for Disease Control and Prevention (CDC) in the United States reported that children who have recovered from COVID-19 may be at an increased risk of being diagnosed with diabetes.
According to The New York Times article, “…The CDC study is among the first to examine large insurance claim databases in the United States to estimate the prevalence of new diabetes diagnoses in children under age 18 who had COVID or were known to be infected with the coronavirus.”
It is important to note that the study—which does not differentiate between type 1 diabetes (T1D), type 2 diabetes (T2D) or any other form of diabetes—only highlights an association born out in the data examined.
The study does not identify how COVID-19 could cause (or provide evidence that it does cause) an increased risk of diabetes in children.
“As a research organization, JDRF will continue to analyze and update our community about these and other data related to COVID-19,” said Sanjoy Dutta, Ph.D., Vice President, Research, at JDRF International. “Other data globally have not shown an association between COVID-19 and diabetes onset, and we are in discussions with clinical leaders to further assess the evidence. In the meantime, we urge the public to be alert to signs of T1D and take steps such as vaccination to protect you and your loved ones.”
How was the study conducted?
The CDC study is based on a summary of findings from two U.S. medical claims databases, IQVIA and HealthVerity.
The examined data from the two databases focused on approximately 500,000 children under the age of 18 years who had a COVID-19 diagnosis between March 1, 2020, and June 28, 2021.
Diabetes incidence in COVID-19 positive individuals was 166 percent higher in the IQVIA cohort and 31 percent higher in the HealthVerity cohort (both compared to COVID-19 negative individuals).
There was no significant difference in diabetes incidence between the age sub-groups or sexes.
Additionally, there is no information in the examined data about other health conditions that could also be associated with a diabetes diagnosis (such as body mass index, blood pressure, etc.). It also does not account for race/ethnicity differences, or comparison with other cohorts that may have differential healthcare access (including less-than-adequate healthcare access).
A similar study has not been conducted in Canada with a Canadian cohort.
Prevention is still the best medicine. Vaccines and T1D
Getting vaccinated is everyone’s best line of defense against severe illness and hospitalization resulting from COVID-19.
All data show the approved COVID-19 vaccines are safe and effective for people with T1D. Vaccines were tested in people with diabetes (9.4% of Moderna,8.4% of Pfizer-BioNTech, and 0.5% of J&J trial participants had diabetes) and no adverse effects were reported in these populations.
Currently, JDRF does not have information on the number of people with T1D in these trials, nor about T1D-specific adverse events reported yet in scientific literature, but there is no evidence now to indicate that these vaccines are unsafe for people with T1D.
Starting in early winter 2021, JDRF Canada successfully advocated that those with T1D be categorized as high priority to receive COVID-19 vaccines, based on data that shows adults who contract COVID-19 and have diabetes experience a three to four times higher risk of severe illness and hospitalization than people without diabetes.
No vaccines yet are approved for children ages 6 months to 4 years, but Pfizer is conducting clinical trials for kids in this age group.
What to do if you have COVID-19 and T1D
If a person with T1D is infected with COVID-19, it can increase the risk for hyperglycemia (high blood glucose levels) and diabetic ketoacidosis (DKA).
DKA can have symptoms that feel flu-like, as does COVID-19. It is essential to continually check blood glucose levels and seek immediate medical attention if any symptoms of DKA are experienced.
According to The New York Times article about the CDC’s data analysis, “Many of the children in the study were only diagnosed (with diabetes) after having an episode of diabetic ketoacidosis (DKA), a (potentially) life-threatening complication that occurs when the body doesn’t have enough insulin to allow blood sugar into cells for use for energy.”
As members of the T1D community know, DKA can be terrifying and is frequently what leads to diagnosis.
To help prevent DKA at diagnosis, it is important to know of the signs of T1D, and see your primary healthcare providers if any of the following are noted:
If you are or a loved one are newly diagnosed with T1D, JDRF Canada has resources and support to help you adapt to your new normal with this disease. Please visit https://breakthrought1d.ca/newly-diagnosed/ for more information, or connect to our Community Engagement team through our support services: https://breakthrought1d.ca/support/
JDRF will continue to monitor research updates about any connection from COVID-19 to T1D and provide more information as it becomes available.
What is the Coxsackie B virus and how does it relate to diabetes?
JDRF is committed to funding the most promising research into cures for diabetes, and better understanding the mechanisms of the disease. One of the most significant challenges of preventing or curing type 1 diabetes (T1D) is that we don’t yet know its causes.
It has been theorized that a viral infection may be partly responsible for triggering T1D. What this means is that a common virus can set off the autoimmune response in the body that results in the beta cells responsible for producing insulin being killed off. This is one piece of the overall T1D puzzle, with certain biomarkers (that can be screened) making a person more likely to have this autoimmune response from a virus. But if we can prevent the virus from taking hold in the first place, we may be able to bring down the number of new diagnoses.
The main virus suspected as a potential cause of T1D is coxsackie B—a common infection that in most circumstances is asymptomatic or has mild symptoms. In rare cases, it may lead to viral meningitis, a heart or brain infection, and hand, foot, and mouth disease.
A potential vaccine
Presently, there are no vaccines against coxsackie B. That said, a year ago, the company Provention Bio started a clinical trial to test a vaccine that they developed against the coxsackie infection.
This trial was the first-in-human study of a coxsackie B vaccine, known as PRV-101, and positive interim results are out. Not only was the vaccine well tolerated by the trial participants (low incidence of side effects), but it induced high concentrations of anti-coxsackie B antibodies – meaning that should someone be exposed to the virus, they would have the means to fight off the infection before it could take hold and prevent triggering the autoimmune response that might cause T1D.
What is JDRF’s role in this vaccine development?
Since the late 1970s JDRF globally has been funding research that seeks to understand the viruses that may lead to the development of T1D. This research has demonstrated that several common viruses can attack islet cells and induce symptoms resembling diabetes.
In 1994, JDRF funded a postdoctoral fellowship for Heikki Hyöty, M.D., Ph.D., working in the lab of Michael Knip, M.D., Ph.D. The project title: “The Role of Coxsackie B and Other Enteroviruses in the Pathogenesis of Insulin-Dependent Diabetes Mellitus.” He went on to show that enteroviruses (of which coxsackie B is a member)—are the main culprit for the development of T1D.
Since this discovery, JDRF has funded Dr. Hyöty with more than 10+ grants, and Dr. Knip with more than 20 grants since 1997.
Hyöty and Knip co-founded Vactech in 2001, which developed PRV-01, and licensed it to Provention Bio in 2017.
In 2017, Provention Bio received an investment from the JDRF T1D Fund to advance the coxsackie B vaccine into clinical trials, and these trials began in December 2020.
What does this mean for people with T1D?
The results released from this study were preliminary; the final results will come in 2022. If the final results remain promising, the next step will be the development of the vaccine from clinic to population, ideally reducing the incidence of T1D diagnoses in children.
This is very exciting news that could prove to be an incredibly useful tool for preventing T1D from ever taking hold with a simple vaccine.
A recent study held in Australia sought to answer the question: for children and adolescents with type 1 diabetes (T1D), does a hybrid closed-loop (HCL) system improve glycemic and psychosocial outcomes compared with conventional management?
The study set out to compare the glycemic control or Time in Range (TIR) and the psychosocial outcomes of a hybrid closed-loop therapy compared to current conventional therapies of continuous subcutaneous insulin infusion (insulin pump) or MDI (multiple daily injections) with or without a continuous glucose monitor (CGM), in children and adolescents with T1D.
“Time in Range” (TIR) is the percentage of time that a person spends with their blood glucose levels in a target range. (“Time in Range | diaTribe”) The range will vary depending on the person, but general guidelines suggest starting with a range of 3.9-10.0 mmol/L. (Over time or in special circumstances such as pregnancy, some people decide to aim for a tighter range, such as 3.5-7.8 mmol/L.)
A HCL system is any insulin pump able to automatically deliver basal insulin by using an algorithm and real-time CGM sensor glucose trends. The HCL system can offer a way of managing diabetes that may improve TIR blood glucose levels; however, it still requires work from the user. (“What is a Hybrid Closed-Loop pump is it for me?”)
Psychosocial outcomes are a combination of physical and social/emotional factors that play a key role in the overall health of an individual. What the study hoped to answer was if a HCL system resulted in better TIR for participants, and if this in turn improved psychosocial health.
Study details?
The study was 6 months long. It was a multicenter, randomized clinical trial with 172 children and adolescents with T1D that took place in 5 pediatric centers in Australia. The study was designed in 2016, recruitment took place in 2017, and the study was completed in 2020.
Eligible participants were randomly assigned to either the intervention or the control group.
The primary outcome was the percentage of TIR between 3.9-10.0 mmol/L. Secondary outcomes included CGM metrics for hypoglycemia, hyperglycemia, and glycemic variability (how much the glucose levels vary). The psychosocial measures were collected using validated questionnaires and included measures such as diabetes-specific quality of life, diabetes distress, treatment satisfaction or fear of hypoglycemia for example.
What were the overall results?
The average age of the participants was 15.3 years and 56% of the participants were female.
In the intervention (HCL) group the TIR increased from a mean of 53.1% per day at the start of the study to 62.5% per day at the end of the study, and from 54.6% to 56.1% in the control group.
The intervention group also had a reduction (-1.9%, 95% CI -2.5% to -1.3%) in the time spent in the hypoglycemic range.
In terms of psychosocial measures, the study found that the HCL system was associated with improved diabetes-specific quality of life. There was no change in diabetes distress scores.
This study is one of the first to report both an improvement in glycemic control (TIR) and quality of life in children and youth using a HCL system in comparison to conventional therapy.
What does this mean for children and adolescents living with T1D?
JDRF advocates patient choice and greater accessibility to diabetes technology, both with blood glucose monitors and insulin delivery systems. While it cannot be universally applied to all individuals with T1D, improved TIR may reduce some of the stress and anxiety surrounding diabetes management, although this study did not show an effect on diabetes distress. These results add to the growing evidence base indicating the positive effects of HCL systems on diabetes management and psychosocial health in young people with T1D. To learn more about JDRF’s advocacy program, please visit www.breakthrought1d.ca/accessforall
JDRF is committed to providing the T1D community with the most up-to-date and relevant information about the ongoing COVID-19 pandemic and its impact on those living with the disease.
As of January 2022, Canada is once again amid what appears to be the worst wave of the pandemic, with the emergence of the Omicron variant. This is not the place we imagined we’d be in the beginning of 2022, nearly a year after the vaccine rollout began and two years into the pandemic. It is a time of understandable uncertainty, fear, and frustration.
While we are undoubtedly exhausted and experiencing pandemic fatigue, until the rate of COVID-19 cases declines, we must continue to take every precaution to try our best to prevent exposure for both ourselves and those in our communities.
Having T1D doesn’t increase the risk of contracting any of the COVID-19 virus variants, but people with T1D – particularly adults – do have an increased risk of serious outcomes if they develop the disease. And Omicron is exceedingly contagious.
Like other COVID variants, Omicron can also be transmitted when a person is asymptomatic or pre-symptomatic, so even if you are feeling fine, it is important to always follow these guidelines to protect yourself and those around you.
Important steps to take to limit exposure
COVID-19 is airborne. This means that tiny virus particles can linger in the air after being exhaled by someone who is infectious. Make sure whenever you leave the house and will be in an indoor setting to have a very well-fitting mask. Ideally, wear an N95 mask which can filter out up to 95% of microbes. If you can’t find an N95, double masking with a medical grade surgical mask (the blue masks you can find at pharmacies) with a tightly fitting cloth mask on top can work nearly as well as an N95. An effective way to check if the mask is tight enough is to wear glasses after you have put on your mask(s) and exhale forcefully. If the glasses fog up, this means air is escaping from the sides or top of the mask. Adjust accordingly until the seal is tight.
Maintain strict hygiene. Wash your hands every time you come home, or after handling/opening a delivery/package etc.
Good ventilation is essential in an indoor setting. Prolonged exposure to aerosolized particles, which are heavier in indoor spaces with low ventilation, significantly increases your risk of being exposed to COVID-19. If possible, avoid spending time indoors anywhere that is not your household, and do not go anywhere without a well-fitted face covering.
Minimize your social interactions and trips outside the house, if possible, and try to avoid busy times or crowds when you do. Always maintain social distancing from non-household members, including while outdoors. Wear masks whenever you are spending time with anyone who is not in your immediate household. This includes receiving deliveries etc.
What should I do if someone in my family with T1D tests positive, or I test positive and have T1D?
If you have COVID-19 symptoms, please contact your healthcare professional. There is a shortage of PCR tests across Canada (nasal swab performed by a healthcare professional and tested at a lab). If you have access to rapid antigen tests, and that test shows you are positive, consider that a confirmed infection. You should then follow public health guidelines on isolation (these differ by province) until you are recovered and symptom-free.
Important steps to take when COVID-19 positive with T1D
COVID-19 elevates the risk of diabetes ketoacidosis (DKA). It is essential to more closely monitor your blood glucose levels and ketones. Making sure you are eating and drinking enough when sick is a challenge. Try and ensure you are eating a balance of protein and carbs and drinking plenty of liquids, even if it’s hard.
Additionally, you are likely taking over the counter medications to help manage your symptoms. Decongestants for congestion and cough can raise blood glucose levels. Suspension (or liquid) medication and cough drops frequently contain sugar.
Some fever reduction medications can be hard on the kidney and liver (like acetaminophen found in Tylenol) and should be taken with caution if you have kidney complications. Aspirin in large doses can lower blood glucose levels. Ibuprofen (found in Advil) can increase the hypoglycemic effect of insulin.
All of this can further complicate blood glucose management.
If you use a continuous glucose monitor (CGM), flash glucose monitor or finger sticks, checking your blood glucose level every few hours can help you better notice any unusual changes. You may also require more insulin. If you can, make sure you have an extra supply on hand.
As well, be extra vigilant checking for ketones (a sign that the body is using fat and muscle for energy, instead of sugar). DKA requires immediate medical attention. An added challenge is the symptoms of DKA can feel flu-like, as do the symptoms of COVID-19. If you notice increased and rapid breathing, and a fruity or sweet smell emanating from the body – this is a sign that the body is trying to rid itself of ketones.
This has been an ongoing time of intense stress. Please ask for help, either from family, trusted friends or a professional if you are overwhelmed. Trying to manage your diabetes along with protecting yourself and your loved ones from COVID-19 is not easy. Speak to your healthcare provider or support network about accessing additional resources and help.