At Breakthrough T1D Canada, we know that living with type 1 diabetes (T1D) is about far more than managing blood glucose levels. Mental health is critical, and T1D affects a person’s emotional, social, and mental well-being throughout their lifetime. Beyond that, people with T1D are at higher risk of mental health disorders including depression, anxiety and disordered eating. These challenges are common among people with T1D and can be treated — but they are often underappreciated or undertreated because of gaps in care and support. Guided by community input, lived experience, and emerging research, our approach aims to raise awareness, reduce stigma, and expand access to meaningful mental health supports for people living with T1D across Canada.
While much of the public conversation around T1D focuses on children and youth, adults with T1D — the majority of the T1D population — face unique and often underrecognized challenges. From the constant cognitive load of daily decision-making to navigating work, relationships, caregiving responsibilities, and long-term health concerns, adults with T1D carry a significant mental and emotional burden. Feelings of burnout, isolation, anxiety, and diabetes distress are common, yet too often go unspoken or unsupported.
Last year, Breakthrough T1D Canada took an important step forward with the release of a video series on our website highlighting the lived mental health experiences of adults with T1D . The series created space for honest conversations and helped shine a light on stories that deserve to be heard.
Building on this momentum, we are excited to announce a new partnership with You’re Just My Type, a nonprofit dedicated to supporting the mental health of people living with T1D through in-person events, resources, and community-building. You’re Just My Type is unique in its focus on reaching underserved areas by hosting free community gatherings in cities across the United States, creating welcoming spaces where people living with T1D can connect, share, and feel understood — regardless of their differences. These gatherings foster understanding, belonging and resilience, by addressing the mental and emotion weight of diabetes.
This partnership will bring You’re Just My Type to Canada for the first time, recognizing the need for initiatives like this and our shared priorities in the importance of fostering social connection and bonding to improve mental well-being. With a proven track record, we know Canadian adults living with T1D will love the in-person and virtual opportunities to take part in these initiatives! Laura Pavlakovich, founder of You’re Just My Type and a person living with T1D was inspired to create the organization. Having lived with the condition for nearly her entire life, she found that the mental toll can often be heavier than the physical.
Laura’s background is in photojournalism, a path that took her all over the world and ignited her passion for storytelling and human connection. In 2016, she began combining these two worlds — photography and T1D — to share the stories of the T1D community. That work eventually grew into You’re Just My Type, where they now focus on building mental-health-centered, peer-led spaces for those living with this condition.
Looking ahead, hosted by YJMT in partnership with Breakthrough T1D will be free, in-person mental health events for adults with T1D, taking place in Vancouver on Saturday May 30, in Toronto later this year, and an online event in the fall. Follow Breakthrough T1D Canada and You’re Just My Type on social media for registration details and updates.
Together, we’re working to ensure no one faces the mental health challenges of T1D alone.
From left to right: Breakthrough T1D Canada staff members Lara Green and Lauren Germain, along with Justice Maki-Chambers and Roslynn Baird, Client Services Administrator, and Godrihwasido (Cayuga “Overseer”), Executive Director of IDHC respectively.
Breakthrough T1D Canada is partnering through a community grant to the Indigenous Diabetes Health Circle (IDHC) to help to address an unmet need with Canada’s Indigenous T1D community.
The grant will help support the development of community informed resources for Indigenous Canadians living with T1D.
Breakthrough T1D had the opportunity to speak with Justice Maki-Chambers, the lead on the project about how it came about and will roll out to improve support and health outcomes for Canada’s Indigenous T1D communities.
Tell us a little bit more about yourself
My name is Justice Maki-Chambers, and I’ve been working as an Eye Health Lead at IDHC for about 3 years. Our Eye Health program focuses on culturally informed approaches to diabetic retinopathy screening in Indigenous communities, in partnership with Vision Loss Rehabilitation Canada (VLRC). On a personal note, I was diagnosed with T1D when I was 16 years old, nearly 10 years ago. Like it is for most people, it was a hard adjustment. This shaped my passion for diabetes education and community-centered health education. Much of my work is grounded in building relationships, supporting self-determination in health, and making sure people have access to the tools they need to stay well.
How did you get involved with IDHC?
When I was working through my Public Health degree at Brock University, I frequently passed IDHC’s head office on my way to and from campus. I had remembered thinking “I am going to work there one day”. Years later, when I was nearing the end of my degree and needed a practicum, I reached out to see if there was any work I could do. Luckily for me, there was. This grew into a contract position within the Client Services Team, and then to a permanent position working on the Eye Health Screening Initiative. IDHC’s commitment to diabetes prevention and management, holistic wellness, and culturally grounded health education is something I’ve admired for a long time, and I am proud to now be a part of. It’s been humbling to contribute to a space where everyone works so tirelessly to uplift Indigenous wellness and create meaningful, lasting change.
Tell us a little bit more about how the IDHC plans to use the community grant to forward the needs of Indigenous diabetes communities in Canada
IDHC has plenty of resources regarding type 2 diabetes, pre-diabetes and gestational diabetes. While these resources can still be beneficial for people living with T1D, there are still important differences to consider, and we would like to support Indigenous individuals living with T1D in the same capacity. We have also had an influx in requests for T1D specific education due to a higher rate of T1D diagnoses in the past few years.
With this community grant, we have developed a Committee of Indigenous people with lived and loved experience to guide the project. We have been doing call outs to have others who live with T1D or are a caregiver of someone who has T1D be interviewed by our committee to hear what kind of resources are actually going to be useful. Once the interviews and surveys are complete, we will use them as a guide to create said resource. Ultimately, we are hoping to create a culturally grounded, accessible and practical and community-informed resource to better support Indigenous people and families living with T1D.
Any further message you want to share with the Canadian T1D community?
As we all know, living with T1D means constantly adapting, learning, and advocating for yourself and others in the T1D community, and this dedication does not go unnoticed. Everyone’s journey with T1D is a little different, but at the end of the day, we all deserve care that respects who we are, where we come from, and the strengths we carry. We deserve access, understanding, and resources that shift with us through our journeys. Chi Miigwech (Thank you) to everyone who has lived with diabetes and has fought for these resources and advancements to make our lives better and thank you to everyone who comes after us to continue this important work.
Surveys to help inform the development of these new materials and resources are available below:
Survey for Indigenous people living with T1D and their caregivers
Danica Doble, a fitness coach and content creator who has been living with type 1 diabetes (T1D) since 2009 recently partnered with Breakthrough T1D Canada as a social media ambassador. She sat down with the organization to share more about her journey, and why she’s so open about how teenage struggles living with T1D empowered her to become a fitness trainer and passionate advocate for the T1D community.
Content warning: please note this piece discusses eating disorders
What do you remember about your T1D diagnosis?
I remember being a seven-year-old little girl and experiencing all of the vicious symptoms that come along with a type 1 diabetes diagnosis. It was a Monday night, and I was at gymnastics practice. Immediately after practice, my mom got a phone call from my doctor stating that I needed to go to the hospital because I had just been diagnosed with T1D. For the next five days, I spent eight hours in the hospital each day and my parents learned everything they could about T1D. Back in 2009, type one diabetes wasn’t talked about much, so my parents really didn’t know what to expect. I remember playing with all the toys that they provided in the hospital and thank goodness for my parents for being attentive, because I most definitely was not. I returned to normal life after those five days, not knowing what was happening to me, not knowing why my parents had to poke my finger and poke my arm every time I wanted to eat. However, as hard as that week was, that week is the reason that I’m who I am today.
Can you tell us a little about starting your fitness journey, after being an active teenager with T1D?
My fitness journey began in 2018; I was like every other teenager. I played sports. I hung out with my friends. I went to school. To be honest with you, I probably lived too much of a normal life. I neglected my blood sugars throughout my teen years and was definitely not focussed on diabetes management. I partied a little too much at times and had a little too much fun with my friends, however, I definitely don’t regret anything because not only did I experience life, but it also prompted me to start my fitness journey.
Although I was quite active as a competitive soccer player, my nutrition was really something that I neglected. After my trip to Europe in 2018, I had told myself that I just wanted to lose 5 pounds to feel better about myself. I quickly learned about calorie deficits and strength training and began doing things to an extreme. 5 pounds later turned into 50. During this time, I had not only lost too much weight but had also lost my period and had developed two eating disorders. It was at this point that I decided to become the healthiest and strongest version of myself. I put on about 20 to 30 pounds, much of it being muscle, and learned everything you could about working out and nutrition.
Can you share a little about your dual diagnoses and how you manage your binge eating disorder (BED) today
My binge eating lasted for about two years, and it was due to the fact that I had eaten so few calories for so long. There were many days when I felt so out of control with my eating and I would compensate these binges by doing hours worth of cardio the next day. It’s an incredibly vicious cycle and very, very difficult to get out of. After my binges, my blood sugars would be so incredibly high, and it would take them hours if not days to come down then the cycle would repeat itself. Today, I am proud to say that I have been free for five years. I started fueling my body properly and made sure that I was getting enough calories. Although I still struggle at times with overeating I no longer eat until I feel sick, which in my opinion is major progress.
How did you come to have food neutrality? My relationship with food has been rocky over the years, but I am proud to say that my relationship with food is at an all-time high. I now understand that there are no good or bad foods and food is food. Some foods are more nutrient dense while other foods are less nutrient dense. However, that does not make one better over the other. Sometimes my body craves a chocolate cake while other times my body is craving a bowl of fruit. In my opinion, I believe that all food serves a significant purpose whether it’s food that makes your body feel good, or food that makes your soul feel good. While the way I physically feel matters, so do memories. I’ve come to realize that food will always be a massive part of celebrations and events, and when I’m 80 years old, I want to be able to look back on these memories and remember all of the laughs that were shared over good food, not how little I ate that day or how healthy I was during these events.
How does powerlifting help you feel empowered with managing your T1D, both physically and emotionally?
Weightlifting has done wonders for me not just physically, but emotionally too. Not only has it significantly helped my blood sugars, but it helped me in so many other aspects of my life. The empowerment I feel from weightlifting is like no other because it just really goes to show that you can do absolutely anything in your life, even with type 1 diabetes.
How do you use your social media platforms to connect with others in the T1D community
I started my social media platforms in 2022 to mainly focus on the fitness side of things however, after about a year, I wanted to do more. I wanted to make an impact for the T1D community and show people that living with it can have positives. I started my type one diabetes account by posting relatable content and bringing light to dark topics quickly. I was able to grow a substantial following on that account and created a community like no other! I’ve connected with hundreds, if not, thousands of people and it is something I will forever be grateful for. I get tons of messages from people telling me that I’ve helped them, when in reality they’ve helped me just as much.
What are you excited about partnering with Breakthrough T1D Canada?
I’m excited to partner with Breakthrough T1D Canada because of the incredible impact the organization has on the type 1 community. I believe that it’s so important to hear stories and experiences from other type 1s, so people know they’re not alone in their experience & journey.
Anything else you’d like to share with the Canadian T1D community?
I’d like to share with the community that as much as diabetes can suck sometimes, and be incredibly difficult, perspective is everything. Type 1 diabetes has connected me with so many amazing people, and it’s made me strong, courageous, and powerful!
Sunday, March 8 is International Women’s Day (IWD), celebrated globally and this year recognizing its 115 anniversary. On IWD we are asked to imagine a world that is truly equal. For that to happen, we need a world free of bias, stereotypes, and discrimination. A world that’s diverse, equitable, and inclusive. A world where difference is not only recognized but also valued and celebrated.
The theme for IWD 2026 is ‘Give To Gain’. Because, when we give, we gain.
The IWD 2026 Give To Gain Campaign encourages a mindset of generosity and collaboration and emphasizes the power of reciprocity and support. When people, organizations, and communities give generously, opportunities and support for women increase. Giving is not a subtraction, it’s intentional multiplication. When women thrive, we all rise.
This theme resonates deeply with Breakthrough T1D Canada, an organization with humble grassroots beginnings, started in the basement of type 1 diabetes (T1D) families desperate to find a cure for their children, but also to raise awareness of what living with this disease is truly like.
From our beginning, we have both supported women, but even more, have been supported by women. From the mothers who demanded more for their children, and their daughters who became some of the T1D community’s fiercest advocates, and who continue to do so today.
To our researchers, many of whom are women, and who continue down the path laid by trailblazing women like Dr. Priscilla White, who was an early pioneer in diabetes research and treatment. Dr. Dorothy C. Hodgkin who first discovered the three-dimensional structure of insulin, Dr. Helen M. Free, who along with her husband created Clinistix, allowing people to check their glucose at home, a significant advance in disease management.
These women played an essential role in advancing understanding of T1D, and the dozens of women researchers we are proud to support today continue this legacy, leading their own critical projects that improve living with T1D and driving us closer to cures. Women researchers can be found in all areas of T1D research, including precision medicine, cell therapy, screening and prevention, disease-modifying therapies, reproductive health and mental health.
Breakthrough T1D also supports a number of women fellows and post-docs, who are leading the next generation of researchers in all areas of T1D research.
To our donors, supporters, volunteers and partners who give tirelessly and selflessly so that these researchers can continue their critical work and get us closer to a world free from T1D. Who with all they give, allow other women to thrive in their field and gain the knowledge needed to make living with T1D safer and better today, while they work towards cures for tomorrow.
To our women-led organization, who are entrusted with the responsibility of stewarding that support with consideration and care.
We have come a long way since the first International Women’s Day 115 years ago, but there is still so much more work to be done. Breakthrough T1D Canada renews our commitment to ‘Give To Gain’ and continue the important work of creating a gender equal world.
Breakthrough T1D Canada is excited to continue its successful partnership with the Canadian Islet Research and Training Network (CIRTN) and announce a fourth cohort of co-funded trainees beginning in 2026.
CIRTN was established in 2020 as a world-class training and research network with joint contributions from the University of Alberta, University of British Columbia, University of Manitoba, Université de Montréal, Institut de Recherches Cliniques de Montréal, and the University of Toronto and now includes 12 institutions from across Canada.
Breakthrough T1D Canada has partnered with CIRTN to leverage funding to this network from the National Science and Engineering Research Council – Collaborative Research and Training Experience (NSERC-CREATE) program.
Dr. Austin Miller –Postdoctoral Fellow (supervisor: Francis Lynn, University of British Columbia) Improving the ability to generate stem cell-derived pancreatic islets in the lab Regenerative medicine approaches are being developed as an alternative in which pancreatic islets are transplanted into patients to restore autonomous insulin secretion, reducing the patient burden of T1D management. Stem cell-derived pancreatic islets (stem cell islets) have the potential to provide an unlimited supply of islets for transplantation.
Overall, my research aims to improve our ability to generate stem cell-derived islets in the lab. I will develop tools to study cellular pathways that allow cells to manage the burden of secreting proteins like insulin and perform studies to better understand the role of these pathways in the generation of insulin-secreting cells. These findings will inform strategies to further improve the efficiency of stem cell-derived islet generation.
Dr. Chris Schaaf – Postdoctoral Fellow (supervisor: Patrick MacDonald, University of Alberta) Standardizing stem cell-derived beta cells The advent of stem cells has provided a promising approach towards generating a functional cure for type 1 diabetes. However, current protocols do not generate stem cell-derived beta cells that appropriately produce and regulate insulin secretion, and there is a lack of standardized assays, benchmarks, and analytical tools for comparing stem cell-derived beta cells to human donor islets.
This project will leverage the humanislets.com dataset – a collection of ‘gold standard’ molecular and functional datasets from hundreds of human organ donors – funded by Breakthrough T1D and CIHR. Using this robust dataset and collaborative expertise in computation and artificial intelligence, we will perform comparative analyses and benchmarking for the improvement of stem cell-derived beta cell outcomes. This will enable us to develop benchmarking standards and protocols that can be used by researchers anywhere in the world to compare their own lab generated stem cell-derived beta cells to our repository of human donor islets data, and use that data to generate stem cell-derived beta cells that truly mimic the function of human beta cells.
Yihan Luo – PhD student (supervisor: Kacey Prentice, University of Toronto) A new approach to prevent type 1 diabetes by strengthening insulin producing cells In the human body, organs communicate with each other through hormones, such as insulin, made by beta cells in the pancreas. Insulin tells fat, muscle, and liver cells to absorb sugar from the blood, which provides energy and keeps blood sugar levels in balance. In type 1 diabetes (T1D), the immune system destroys betacells, causing lifelong insulin deficiency. Evidence suggests that T1D begins before beta cell loss, due to disrupted insulin responses and organ–pancreas communication. Fabkin, a hormone complex secreted by fat, affects beta cell health and research has shown that blocking it in mice helped betacells stay healthier. Our project studies Fabkin’s key component, NDPK, to learn how it affects beta cell survival and function, and test whether NDPK-targeting drugs can prevent or delay T1D. If successful, this work could lay the foundation for a new approach to prevent T1D by protecting beta cells before they are damaged or lost.
Stephanie Atkinson, a Montreal, QC based adult Breakthrough T1D Canada ambassador, sat down with the organization to discuss what drew her to volunteering and what it’s like to be diagnosed as a busy mother and businesswoman.
Tell us a little bit more about yourself
My name is Stephanie Atkinson. I’m a mom of four, a skin and beauty expert, founder of Mayfield Glow, and a recent finalist on the Miss Universe Canada stage.
Before anything else, I’m someone who has learned firsthand how fragile life can be — and how powerful resilience is.
I built my career helping women feel confident and cared for through skincare and wellness. But my own health journey shifted my purpose in a deeper way.
Standing on the Miss Universe Canada stage as one of the first finalists openly wearing two visible diabetes devices — an insulin pump and a continuous glucose monitor — wasn’t just about competing. It was about representation. It was about showing that living with a chronic illness does not disqualify you from showing up fully, boldly, and beautifully in the world.
Today, I use my platform to advocate for type 1 diabetes awareness, especially for adults diagnosed later in life, while balancing motherhood, entrepreneurship, and advocacy.
Can you share a little bit about your diagnosis? What do you remember?
Before my diagnosis, I was sick for many days, but it was during COVID and most clinics were closed, so accessing care felt nearly impossible. I was exhausted in a way that didn’t make sense. I now know I was experiencing all the classic “4 Ts” of type 1 diabetes — thirst, tiredness, toilet, and thinner. I was constantly thirsty, extremely fatigued, using the bathroom nonstop, and losing weight rapidly. My vision began to blur, I could barely walk, and deep down I knew something was very wrong — but as a mom, you push through.
When I finally got into a clinic, I was told I had a urinary tract infection. I remember saying I had never had one before, but I was told that strange things happen before turning 30. I left feeling dismissed, even though my body was telling me something much more serious was happening.
The next morning, everything changed.
I woke up to a police officer at my door doing a wellness check. My doctor had reviewed my results and realized I had been misdiagnosed — my blood work showed I was actually in diabetic ketoacidosis (DKA), a life-threatening emergency where the body begins breaking down fat for fuel because it cannot use glucose properly without insulin. Acid builds up in the bloodstream, and without immediate treatment, it can be fatal.
When I got to the hospital, things were still confusing. Initially, I was diagnosed with type 2 diabetes because I was an adult. But my condition worsened quickly, and I ended up in the ICU with severe DKA. I remember feeling like my body was shutting down. I was losing vision in my left eye, I couldn’t walk properly, and everything felt overwhelming and terrifying.
Later, after further testing, I was correctly diagnosed with type 1 diabetes.
I was 29 years old, a mother, and suddenly my entire life changed. I didn’t fit the stereotype people imagine when they think of Type 1 diabetes — and that experience is one of the main reasons I advocate so strongly today, especially for adults who are diagnosed later in life.
Over 70% of Canadian T1D diagnoses are in adults. How did you find the transition to your new normal?
The hardest part wasn’t just learning how to manage insulin — it was realizing how little support exists for adults diagnosed later in life.
As a mother and entrepreneur, I had to quickly learn how to balance blood sugars, medical appointments, and new technology while still showing up for my family and my work. There’s a lot of education and community built around children diagnosed with Type 1, but adult diagnosis can feel isolating.
To be honest, there were many times I wished I had been diagnosed as a child. By the time I was diagnosed, I was already an adult, already a mom, already carrying so many responsibilities. A lot of guilt came with that — guilt about how my diagnosis might affect my family, guilt about slowing down, and guilt about having to suddenly prioritize my health in ways I never had before.
Over time, I learned that managing diabetes isn’t selfish — it’s necessary. I built a support system, connected with community, and learned to use technology as a tool for confidence instead of fear. That transition taught me how strong and adaptable we really are, and that being diagnosed later in life doesn’t mean you’re behind — it just means your journey looks different.
You went into DKA prior to your diagnosis. Are ketone levels and how they’re measured something you think about more now?
Absolutely. Once you’ve experienced DKA, awareness becomes second nature.
I pay close attention to how my body feels, especially when blood sugars are elevated or when I’m sick. I monitor ketones when needed and rely heavily on my diabetes technology for early warnings. It’s not about living in fear — it’s about understanding my body and staying proactive so I can avoid going through that experience again.
Why do you wear your diabetes devices so visibly?
The honest answer is that at first, I didn’t want to.
In the beginning, I was ashamed of my devices and tried to hide them as much as possible. As a woman working in beauty and wellness, I felt pressure to look polished and seamless, and I worried that people would only see my diagnosis instead of me.
What changed my perspective was my children.
One day, one of my kids came home from school excitedly telling me about a student in their fifth-grade class who wore a Dexcom and was having a diabetic emergency. Because my child was familiar with diabetes from watching me manage it every day, they recognized what was happening and were able to help alert an adult quickly.
That moment shifted something in me. I realized this was bigger than me. If more people saw these devices visibly — and understood what they were — it wouldn’t just help me feel more confident, it could help others too.
On the Miss Universe Canada stage, I made a conscious decision not only to wear my devices openly, but to bedazzle them. So many times, I hear, “But you don’t look sick.” And the truth is — Type 1 diabetes is an invisible illness. I wanted to bring joy and light to something that can feel heavy and misunderstood. If I was going to wear them, I was going to wear them proudly.
Visibility creates conversation. Conversation creates understanding. And understanding saves lives.
If someone sees me and feels less alone or more confident wearing their own devices, that makes it all worth it.
Is there anything else you wanted to share with the T1D community, particularly with others diagnosed as adults?
You did not cause this.
Being diagnosed as an adult can feel confusing and isolating because many people still believe type 1 diabetes only happens in childhood. When you’re diagnosed later in life, you’re often already carrying so many responsibilities — careers, families, and expectations — and it can feel like your world shifts overnight.
But your diagnosis does not change your value, your strength, or your future.
Give yourself permission to learn slowly, to ask for help, and to prioritize your health without guilt. Managing diabetes isn’t about being perfect — it’s about showing yourself grace and continuing to move forward.
You can still chase your dreams. You can still show up boldly. You can still build a beautiful, full life. Type 1 diabetes is something I manage — it does not define or limit who I am.
***
Breakthrough T1D Canada thanks Stephanie for her efforts on behalf of the T1D community and for her important work as a peer support volunteer and advocate.
What does a cure for type 1 diabetes (T1D) look like?
Authors: Katie Bartel, Beth Miller, Tony Lucas, Benjamin Mammon, forThe Breakthrough T1D Canucks For Kids Fund Centre of Excellence at UBC T1D Lived Advisory Group
That was the question that the Type 1 Diabetes Lived Experience Advisory Group attempted to answer through a recent anonymous survey.
The group quickly learned it’s not an easy puzzle to solve.
The Breakthrough T1D Canucks For Kids Fund Centre of Excellence at UBC T1D Lived Advisory Group has a key role at Centre outreach events and enabling dialogue between researchers and people living with T1D. The recent survey was done to gather information to inform these discussions and, in turn, the Centre’s cure-focused research program.
Of the 49 respondents, there were varying degrees of what a cure for T1D looks like – some want fully functioning insulin production, whereas others would be satisfied with a device-free lifestyle. Some respondents focused more on improved quality of life, while others struggled to put any kind of description to a T1D cure.
“Type 1 requires so much decision making on a daily basis that I cannot help but wonder what my brain will do with that space and time,” one participant commented. “Am I less likely to face decision fatigue? More likely to have more resilience to frustration… the potential is significant, but the ability to guess what that might be is difficult.”
It’s these types of responses that the Centre’s T1D Advisory Group believes is essential for researchers to know.
“If we don’t know what a cure looks like for people with type 1 diabetes, we can’t work towards it,” said Dr. Søs Skovsø, scientific project coordinator at the Centre, and Chair of the Advisory Group.
And that’s where the Advisory Group plays a role.
The Advisory Group is made up of eight members who either live with T1D or care for people living with T1D. The group’s objective is to integrate the voices of people with T1D into T1D research.
The Advisory Group developed a survey that was distributed through local T1D community networks and stayed open for one month. There were 49 respondents in total; 33% were caregivers and 67% lived with T1D. Most respondents lived in Canada – 53% in BC and 41% in other provinces. The remaining 6% lived internationally.
The main query of the survey was “What does a cure for T1D mean for you?”
Questions included rating the importance of restoring the body’s ability to produce its own insulin again, versus preventing the immune system from attacking insulin-producing cells. The survey asked about the importance of a cure being device free, as well as the significance of improvements to quality of life gained with the introduction of a cure.
51% of survey respondents responded that a cure involving stem cell therapy would be extremely important; 58% rated immune therapy as extremely important; and 40% rated being device-free as extremely important. And when asked about the most important benefit that a T1D cure could provide – improved mental health was rated higher than freedom from blood sugar checks, elimination of insulin dependence, and reduction of long-term health risks.
The question that was most surprising for Advisory Group members and researchers at the Centre was how confident respondents were that a cure would be found in their lifetime.
Responses varied: some were confident, others skeptical.
“The mixed response from the community doesn’t reflect the exciting work that’s going on at the Centre,” said Advisory Group member Beth Miller. “This highlights a need for better communication between the scientific community and the broader T1D community,” Miller added.
Skovsø agrees.
“Some people have lost hope for a cure, and at the same time others thinking that there’s a cure coming next year,” she said. “This means that the research community has to do a better job at communicating that a cure may not be available next year, but it is within reach.”
The Advisory Group’s survey is the first of its kind according to Dr. Bruce Verchere, one of the lead principal investigators at the Centre.
“This survey promises to increase the impact of T1D research in the Centre by helping researchers better understand the hopes and expectations of persons living with T1D, and how research could improve their lives,” said Verchere.
“What a cure looks like to a parent of a child with T1D, or to someone living with T1D for 30 years, or to a scientist is going to be different,” said Skovsø. “Hopefully this survey will help open minds that a cure is not single-sided; it’s multi-faceted.”
This survey was just the first step. A second quantitative survey is now being developed by the Advisory Group, in collaboration with the Centre research team, with the intent of reaching a wider audience and publishing the results in a scientific journal.
“It’s cool to see the work and conversations coming out of the Advisory Group trickle and spread into the science community,” said Skovsø. By publishing a larger study, “we can spark even more conversation and understanding.”
Do you prefer the sweetness of a Hershey’s kiss, or maybe you like the spice of a cinnamon heart? For most of us, we can grab a handful of Valentine’s Day candy without thinking about it. But for people living with type 1 diabetes (T1D) every snack, every meal, every piece of food eaten must first be calculated for carbs and sugar against the insulin they need to take – just to stay alive.
For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.
Always make sure to check the label carefully, and consider downloading an app, like Roche’s mySugr app, Diabetes M, or apps from your device manufacturers. Visit the website of the manufacturer of your device to find out more.
Carbs and Calslets you take a photo of your meal, and the app searches its library of over 19,000 foods to give you the nutritional information you need.
MyFitnessPal app includes a database of over 14 million foods so you can find out nutritional information about what you’re eating, including the amount of carbs. It has a handy barcode scanner for ready-made products, and you can also add your own foods.
There is a free version and a paid version which has more features. The app is compatible with iOS and Android.
We always want the holidays to be fun for you, or a loved one with T1D, knowing that treats can still safely be enjoyed. It just requires a little extra work and knowing the carb levels of favourite candies.
Remember also to factor in the portion of candy or chocolate you or your child eats to get a more accurate carb count.
Great Value Cinnamon Hearts (25 pieces) contains 15g total carbs, 15g net carbs, 0g fat, 0g protein, and 60 calories.
Hershey Kiss (1 piece) contains 3g total carbs, 2.8g net carbs, 1.5g fat, 0.4g protein, and 27 calories.
Hershey’s Reese’s Peanut Butter Cup (1 package – each 1.5 OZ – 2 cups – 2 1/8″ diameter per cup) contains 23g total carbs, 21.7g net carbs, 12.8g fat, 4.3g protein, and 216 calories.
Jellybeans (10 piece) contains 28g total carbs, 28g net carbs, 0g fat, 0g protein, and 113 calories
Compliments Jujubes (8 candies) contains 33g total carbs, 33g net carbs, 0g fat, 0g protein, and 130 calories.
On January 20, 2026 Novo Nordisk (“Novo”) and Vancouver-based Aspect Biosystems (“Aspect”), announced a new phase of their partnership focused on developing curative cell therapies for type 1 diabetes (T1D).
Since 2023, Aspect and Novo have worked together on technologies aimed at producing insulin-secreting islet cells from stem cells. Under the revised partnership, Aspect has acquired Novo’s stem cell–derived islet and hypoimmune cell engineering technologies—designed to create insulin producing cells that can evade immune attack after transplantation into people with T1D.
Novo will continue to invest in Aspect and provide research funding, and it will retain future commercialization and royalty options. This agreement follows Novo’s October 2025 decision to discontinue its cell therapy research and development, including but not limited to, T1D islet manufacturing. As part of the transition, T1D-related research, development, and manufacturing activities will move from the U.S. and Denmark into Aspect’s Canadian platform, expanding the company’s domestic capacity.
This milestone further strengthens Canada’s leadership in T1D research and builds on the $73M Federal–Provincial (BC) investment in Aspect announced in July 2024.
What does this mean for Canadians with T1D? To cure T1D, we need to do two things: we need to protect insulin-producing beta cells from autoimmune attack, and we need to protect and restore their function. To achieve this requires developing a renewable source of cells, as well as therapies that don’t require immunosuppression, as with traditional organ and tissue transplants.
This partnership will help advance cure research that is advancing on both fronts towards the ultimate goal of freedom from insulin, for people of all ages with T1D. And it will be taking place right here in Canada.
Ramya (left), Dr. Bruce Verchere, Co-Director at the Centre (middle), and Dr. Benjamin Mammon, another member of the T1D Lived Experience Advisory Group (right). Photo credit: Macy Yap
Type 1 diabetes stories help shape research
Ramya Hosak was diagnosed with type 1 diabetes (T1D) at age 19 while attending university. Since then, she has been a devoted volunteer, helping others navigate the challenges of T1D and the steep learning curve that accompanies a life-altering diagnosis.
As co-chair of the T1D Lived Experience Advisory Group at the Breakthrough T1D Canucks For Kids Fund Centre of Excellence at the University of British Columbia (UBC), her perspective helps guide the Centre’s research and connect the T1D community with the researchers advancing cures. Her voice is just one of many representing a diverse group of faces and stories, working with researchers to drive innovative therapies.
Ramya’s passion is nonprofit work, specifically in social justice, community development, and equal access to healthcare. To better unite the T1D community in BC, she co-founded Young and T1, a local support group that helps young adults with T1D through the transition to adulthood.
We asked Ramya to share the reasons behind her incredible volunteering and what T1D research means to her.
Breakthrough T1D Canada: Can you tell us about your T1D diagnosis?
Ramya: I was diagnosed in my second year of university. Super tired and barely able to keep my eyes open in the lecture hall, I was constantly chastising myself. “Don’t be a wimp, everyone else is struggling with midterms and finals, get it together and toughen up, Ramya,” I thought to myself as I chugged a litre of juice.
But I kept getting weaker. Eventually, my parents dragged me to the hospital, practically carrying me to the ER. That’s when I found out, at 19 years old, that T1D can occur at any age, not just in childhood. Initially, I was relieved at the diagnosis that explained my recent exhaustion. Yet as time went on, questions arose that couldn’t be answered by medical professionals who hadn’t been in my position. My parents and friends assumed that as a responsible adult, I had things under control and was fine.
But I wasn’t fine. I went from being a student who enjoyed an active social life, going out with my friends without a second thought, to suddenly having to be so careful. I felt a need to act like everything was fine and hide the toll that the invisible full-time job of T1D was having on me, mentally and emotionally.
I stopped reaching out to my friends for fear of being seen as a complainer and not having a positive attitude. I went through a period of extreme depression, feeling like no one “got me.” But after graduating from university, I started getting better and began meeting others my age with T1D.
Breakthrough T1D Canada: What drew you to participate in the Centre’s T1D Lived Experience Advisory Group?
Ramya: My undergraduate degree was in Health Sciences, and research has always held an interest for me, particularly as my mom is a cancer researcher. I’ve grown up hearing about her excitement, disappointments, and long days/nights that come along with being a researcher. I respect this work immensely, and to be able to work with researchers who are working so hard to find a cure for diabetes and bridge the gap for those living with T1D has always been very important to me. Similarly, I love the questions researchers ask me about living with T1D and helping them to understand why their hard work truly matters.
Photo credit: Macy Yap
Breakthrough T1D Canada: How do you feel about the cure research happening at the Centre?
Ramya: Excited! Not just for me, but for the future generation! I truly believe a cure is in sight, and having had my first child recently (September 2025), the potential to eliminate T1D in the generations to come is such a wonderful thought.
Breakthrough T1D Canada: What research excites you most?
Ramya: I find Dr. Megan Levings’ work on immune system regulation as it relates to T1D particularly interesting. I work at the Kidney Foundation of Canada and have seen her work in the transplant field come up as well. It’s exciting to see research in immunology having the potential to lead to additional breakthroughs in other health-related issues.
Breakthrough T1D Canada: What are your hopes for the future of diabetes?
Ramya: My hope is that within the next generation, T1D markers can be identified in at-risk patients before disease onset or at early onset, and the correct therapies can indefinitely prevent it from fully taking place (by preserving remaining beta cell function, etc.).
“The real glory would be never having to carb-count, constantly be checking my blood levels and worrying about how every variable of life impacts my glucose numbers and therefore how I feel physically and emotionally throughout the day with this 24/7 invisible job. So much mental space would be freed up.”
Ramya with her husband, Mark, who also lives with T1D (diagnosed at age 10), and their newborn daughter.
Breakthrough T1D Canada: What prompted you to launch Young and T1?
Ramya: Upon diagnosis, I started volunteering for Breakthrough T1D (then JDRF), and when working with youth ambassadors, it was so amazing to hear kids meet other kids who shared the same diagnosis. They told stories of bullying at school when their pumps were seen as strange, compared pump colours with each other, and it was just so normal.
I really wanted a community that “got” what living with T1D in adulthood felt like. T1D gets lonely. I hear this a lot. Young people at this transition stage often feel uncomfortable speaking with their doctor or parents about complex issues that arise for an adult with T1D. Thirteen years ago, I did not realize what an awesome resource Young and T1 would be—for myself and now over 700 individuals in BC—for learning and sharing with one another.
Through meeting folks with similar daily struggles, and living with my husband Mark, who also has T1D, I have learned that all bodies are different. One size does not fit all in T1D management, and getting as much information available to us as possible is important. By conveying our struggles and successes with one another, we all benefit from shared knowledge.
—
Breakthrough T1D Canada is grateful to Ramya for sharing her story and helping our researchers accelerate breakthroughs. Knowledge sharing is critically important not just among the T1D community but also among the researchers who will one day bring cures to the community.
Breakthrough T1D oversees T1D research worldwide to ensure that teams are collaborating and sharing learnings. The Breakthrough T1D Canucks For Kids Fund Centre of Excellence at UBC is a prime example of that collaboration in action, with over 40 multidisciplinary researchers working together to tackle all angles of cure research.
The Centre is a key pillar of our $100M Campaign to Accelerate, a national campaign with a global impact. Read about research highlights from year 4 of the Centre’s three interconnected research themes advancing cures here.
Philanthropic donors are advancing promising cure research in BC and around the world. To learn more about these exciting projects or to make a leadership gift, please contact:
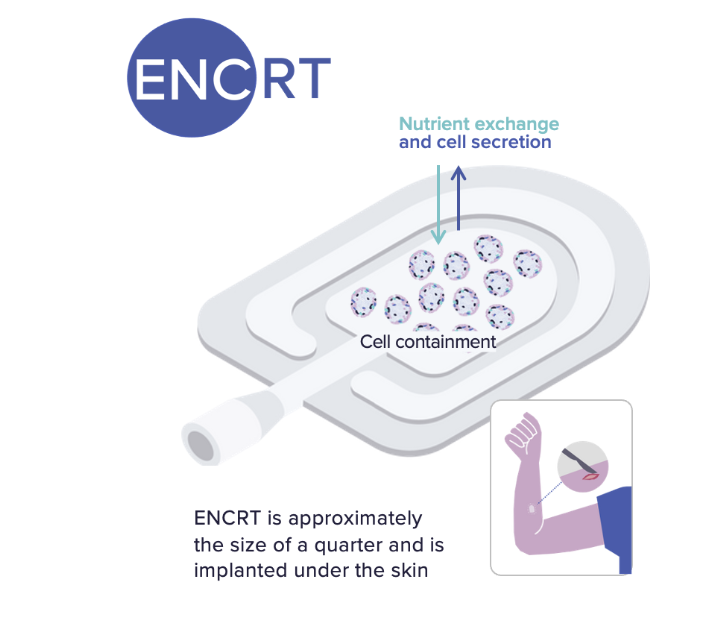
On January 6th, 2026, Encellin (California, Quebec) reported positive interim results of its Phase 1 clinical trial of encapsulated islets in people with type 1 diabetes (T1D), which is being carried out in Toronto and Montreal.
Trial Details: In Encellin’s trial, cadaveric human donor islets are being encapsulated in Encellin’s Encapsulated Cell Replacement Therapy (ENCRT) device and implanted into adults with T1D. This first-in-human trial is assessing (1) safety and adverse events, (2) cell survival within the device, and (3) fibrosis, or scarring, around the implants.
Interim Results: As planned, ENCRT devices were removed from the initial five participants after 4 months of implantation. Analysis of the removed devices show:
minimal to no fibrosis (formation of scar tissue around the device);
robust formation of blood vessels around the device;
viable islets inside the device.
These results indicate that the device has the potential to host islet cells while maintaining sufficient oxygen and nutrient flow for the cells to work effectively.
Historically, macroencapsulation devices (which act like a teabag to enclose the islet cells) have had limited success due to high levels of fibrosis that prevents cell survival, reduces the ability of the cells to access oxygen and nutrients, and limits the release of insulin. The preliminary finding that fibrosis is not occurring with Encellin’s device is therefore a critical step toward overcoming the barrier of fibrosis with islet encapsulation devices and advancing the development and delivery of cell-based therapies for people with T1D.
We will continue to report updated results as they become available.
Breakthrough T1D’s Role: Encellin’s technology was originally developed within the Lab of Dr. Tejal Desai (University of California San Francisco) with funding from Breakthrough T1D, which was crucial in the formation of Encellin as a company and attracting subsequent venture capital.
While we look forward to the year ahead, we want to also reflect on 2025 and the breakthroughs we saw, in type 1 diabetes (T1D) research, advocacy, community engagement, and more. We were also able to host successful events and community initiatives across the country.
Our first full year as Breakthrough T1D Canada was one of impact. And while we may have a new name, our mission and commitment to the T1D community didn’t change; it was only strengthened.
Our incredible community of donors, volunteers, and supporters are the heart and soul of everything we do, and thanks to them it was a transformative year. We committed substantive funding to research, further developed partnerships in academia with new fellowships and grants, continued to support newly-diagnosed people, and our adult T1D community, reinforcing our commitment to being a source of trusted information and support to all Canadians affected by T1D, at any age and any stage of their journey with this chronic disease.
Curing T1D is and remains our north star, while we work to improve the lives today of the estimated 300,000 Canadians with T1D until we have a world free from type 1 diabetes.
Launched ‘Beyond the Numbers’, a compelling video series that features real stories about mental health challenges and T1D
Seeing improvements in device access in Newfoundland and Labrador and Saskatchewan, while continuing to advocate to other provincial and federal governments for increased support
Reaching thousands of Canadians impacted by T1D through our Breakthrough T1D Education Series, bringing experts into their homes to discuss topics important to them.
Thanks to donors to the $100M Campaign to Accelerate, the Breakthrough T1D Canucks For Kids Fund Centre of Excellence at UBC marks four years of innovation
Continuing a successful partnership with the Canadian Islet Research and Training Network (CIRTN) and announced a third cohort of co-funded trainees
Vertex FORWARD trial of Zimislecel (previously called VX-880) is currently the most advanced stem cell-derived islet replacement trial. Of the 12 individuals that have reached the one-year mark post-transplant, all have resolved severe hypoglycemic events, reduced HbA1c to 7% or less, and 10 of 12 are off insulin
In disease-modifying therapies:
Interim results presented from Sanofi’s PETITE-T1D trial demonstrated acceptable safety of Tzield in kids aged 0-7 with early-stage T1D
To read more about research updates and stories of people living with T1D, please visit www.breakthrought1d.ca/blog.
As we head into 2026, we pause and reflect on how truly grateful we are for the support of our donors, volunteers and the commitment of the T1D community. We’re very excited to approach this new year with renewed vigour, working to build on these breakthroughs and continuing to push our mission forward.
And thanks to your generosity, cures have never been closer.











 For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.
For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.  There is a free version and a paid version which has more features. The app is compatible with iOS and Android.
There is a free version and a paid version which has more features. The app is compatible with iOS and Android.